Delusions: Definition, Causes, & Examples
When do beliefs become delusions? Keep reading to find out.

*This page may include affiliate links; that means we earn from qualifying purchases of products. |
We all have beliefs about the way the world works. Some of our beliefs are accurate, some are comforting, and others may be misguided. Regardless of how closely our beliefs correspond to reality, we don’t typically consider them pathological. So where do we draw the line between beliefs and delusions?As with many psychiatric disorders, the border between “normal” and pathological isn’t perfectly clear. A monk might strongly believe he is receiving commands from God and we wouldn’t try to get help for him. On the other hand, a person in a convenience store having an audible conversation with God about what candy bar to buy might cause some alarm. Although the distinction here between normal and abnormal is challenging to articulate adequately, there are some important differences between beliefs and delusions. Let’s talk more about what delusions are and where they come from.
|
Are You a Therapist, Coach, or Wellness Entrepreneur?
Grab Our Free eBook to Learn How to
Grow Your Wellness Business Exponentially!
✓ Save hundreds of hours of time ✓ Earn more $ faster
✓ Boost your credibility ✓ Deliver high-impact content
What Are Delusions? (A Definition)
Within the research community, there are three commonly cited characteristic features of delusions (Feyaerts et al., 2021).
- The content is false or impossible
- It is held with unshakable conviction
- It persists despite rational argument or overwhelming counter-evidence
Causes of Delusions
Delusion Cause: Biological Factors
Delusions may result from changes in brain chemistry or structure, such as abnormalities in dopamine or glutamate levels, or brain damage due to injury or disease.
Delusion Cause: Genetics
There may be a genetic predisposition to developing delusions, as certain genes have been linked to an increased risk of developing schizophrenia and other psychotic disorders.
Delusion Cause: Psychological Factors
Delusions may be a result of certain psychological conditions, such as low self-esteem, paranoia, or severe anxiety.
Delusion Cause: Substance Abuse
The use of certain drugs, such as hallucinogens, amphetamines, and cannabis may trigger or exacerbate delusions.
Delusion Cause: Environmental Factors
Trauma, stress, and other environmental factors can trigger delusions in vulnerable individuals.

Examples of Delusions
Type of Delusion: Persecutory
Persecutory delusions involve the persistent anticipation of possible future danger that cannot be resolved. People who are suffering from persecutory delusions often demonstrate a great deal of anxiety and worry, and they have the tendency to jump to conclusions. Someone with persecutory delusions might feel like they are constantly being surreptitiously monitored by a nefarious agent or that their friends are conspiring against them. This type of delusion is the most commonly observed for many types of psychosis (Freeman, et al., 2002).
Type of Delusion: Alien Control
Delusions of alien control are understood as the misattribution of self-generated actions to an external source, such as aliens. People suffering from this type of delusion experience their thoughts, speech, and actions as being influenced or replaced by those of external agents rather than attributing them to themselves (Blakemore, et al., 2003). For example, someone suffering from the alien control delusion might experience the act of driving their car as a decision they did not make and behavior that is beyond their control.
Type of Delusion: Grandiose
Grandiose delusions, also referred to as delusions of grandeur, involve having an inflated sense of worth, power, or knowledge, or having a special identity (Knowles et al., 2011). This is an example of something an individual with grandiose delusions is reported to have said:
“I would write books on psychiatric theory… on theology. I would write novels. I had the libretto of an opera in mind. Nothing was beyond me… The major work which would be based on this material would be accurate, provocative, and of profound significance.” (Goodwin & Jamison, 2007).
Type of Delusion: Thought Broadcasting
People suffering from this delusion believe that their thoughts can be accessed by others and are being broadcasted or transmitted to others without their knowledge or consent through means such as telepathy, radio waves, or other electronic signals (Pawar et al., 2002). This delusion can be exceptionally distressing and lead to paranoia and isolation.
Type of Delusion: Religious
Religious delusions are a type of delusion that involve beliefs or experiences related to religious or spiritual themes. These delusions can occur in individuals with various mental health conditions, such as schizophrenia, bipolar disorder, or major depression, among others.
Examples of religious delusions may include (Siddle et al., 2002):
- The belief that they are a religious figure.
- The belief that they have been chosen by God for a special mission or purpose.
- The belief that they have special religious powers or abilities, such as the ability to heal or perform miracles.
- The belief that they are possessed by demons or evil spirits.
- The belief that religious symbols or texts have a special meaning or significance specifically related to themselves. (Siddle et al., 2002).
Type of Delusion: Guilt
People suffering from delusions of guilt believe that they are responsible for a particular event or situation without any evidence to support this belief. They often believe that they have committed a serious offense or sin and that they are deserving of punishment. They may also believe that they are responsible for events or situations that are outside of their control, such as natural disasters or accidents (Kiran & Chaudhury, 2009). For example, someone with this delusion might feel that they were responsible for Hurricane Katrina.
Type of Delusion: Somatic
Somatic delusions are also called monosymptomatic hypochondriacal psychosis (Joseph & Siddiqui, 2022). People with somatic delusions believe that they have a serious medical condition, despite medical tests and evaluations indicating otherwise. They may also believe that they are experiencing physical symptoms that are not present or exaggerated, such as pain, burning sensations, or unusual smells, and are unarguably convinced of the severity of their symptoms. The most common type of somatic delusions is that they are infested with parasites, body dysmorphic delusion, and body odor or halitosis.
Delusions vs Hallucinations
Delusions and hallucinations are related concepts. For example, both delusions and hallucinations involve inaccurate perceptions of reality and both can be highly distressing. Hallucinations are also common in people with delusions, especially when caused by psychosis. However, they are different in several important ways.
One of the most essential differences is that hallucinations are sensory experiences whereas delusions are beliefs. That is, hallucinations include sensations such as feeling touch or movement on your skin, hearing voices, seeing something that isn’t there, smelling something that isn’t real, and feeling like you are floating. In contrast, delusions might include cognitive interpretations or beliefs about these sensory experiences. For example, someone might have a hallucination in which they are hearing voices and have the delusion that these voices are aliens talking to them telepathically. Additionally, hallucinations are typically transient while delusions are persistent (Langdon & Coltheart, 2000).
Delusions vs Illusions
Another important distinction is that illusions are a common occurrence in healthy people and are simply a byproduct of how the brain works. Our brains are essentially prediction machines that have learned over time how the world works and what we can expect as we move through it. These predictions influence our sensory experience in such a way that we are more likely to have the experience we predict than the one that aligns with reality.
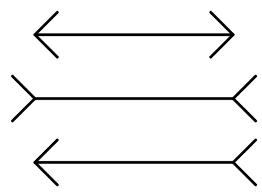
Visual illusions are a common example of how we see what we expect over what is there. One popular visual illusion is the Muller-Lyer illusion. Given how we typically experience the world and what our brains expect we see one of these lines as longer than the others. However, in reality, all the lines are the same length.
Delusions vs Paranoia

Delusions vs Delirium
Delirium is a state of confusion and disorientation associated with changes in attention, awareness, and other cognitive processes that is typically temporary. Delirium can be caused by a variety of factors including neuroinflammation, brain vascular dysfunction, altered brain metabolism, imbalance of neurotransmitters, and impairments in the networks of neurons that support cognition. These pathological changes could be triggered by drug consumption or withdrawal, trauma, surgery, or other medical conditions (Wilson et al., 2020).
The key difference between delusions and delirium is that delusions involve false beliefs that are persistent, while delirium is a temporary state of confusion. Additionally, delirium may be caused by drug use or medical conditions whereas delusion isn’t necessarily associated with acute physiological changes such as these.
Treatment for Delusions
Cognitive Behavioral Therapy (CBT) is another common treatment for delusions (Mehl et al., 2015). CBT is a form of psychotherapy that focuses on the formation and maintenance of these thoughts, feelings, and behaviors. This has been shown to be an effective treatment for delusions for most people (Mehl et al., 2015). The use of CBT for delusions is based on the premise that psychotic and normal experiences exist on a continuum, which suggests psychotic experiences, like delusions, might be amenable to psychological treatments that are effective for healthy people (Mehl et al., 2015).
Quotes on Delusions
- “The belief that one’s own view of reality is the only reality is the most dangerous of all delusions.” – Paul Watzlawick
- “No man is happy without a delusion of some kind. Delusions are as necessary to our happiness as realities.” – Christian Nestell Bovee
- “The house of delusions is cheap to build but drafty to live in.” – A. E. Housman
- “Every journey into the past is complicated by delusions, false memories, false namings of real events.” – Adrienne Rich
- “Our mind is like a cloudy sky: in essence clear and pure, but overcast by clouds of delusions. Just as the thickest clouds can disperse, so, too, even the heaviest delusions can be removed from our mind.” – Kelsang Gyatso
- “He had delusions of adequacy.” – Walter Kerr
- “Schizoaffective disorder is a big mental mash-up of a disease. It combines just about every disorder, from depression, delusions, and paranoia to mania, schizophrenia and hallucinations. My mother bounced between all of these regularly while raising me alone in our Hollywood home.” – Shawn Amos

Articles Related to Delusions
Books Related to Delusions
Final Thoughts on Delusions
Delusions can be a painful and distressing symptom of neuropsychiatric disorders. They are a challenging symptom to treat because they manifest in a variety of ways that are dependent on a combination of several different factors like genetics and culture. Though the beliefs associated with delusions are resistant to change, even in the face of overwhelming evidence, research suggests that they may be treatable with CBT. For more on delusions, check out this video:
Video: Examples of Delusions | How are Delusions Treated?
Don’t Forget to Grab Our Free eBook to Learn How to
Grow Your Wellness Business Exponentially!
References
- Bell, V., Halligan, P. W., & Ellis, H. D. (2006). Explaining delusions: a cognitive perspective. Trends in cognitive sciences, 10(5), 219-226.
- Corlett, P. R., Taylor, J. R., Wang, X. J., Fletcher, P. C., & Krystal, J. H. (2010). Toward a neurobiology of delusions. Progress in neurobiology, 92(3), 345-369.
- Feyaerts, J., Henriksen, M. G., Vanheule, S., Myin-Germeys, I., & Sass, L. A. (2021). Delusions beyond beliefs: a critical overview of diagnostic, aetiological, and therapeutic schizophrenia research from a clinical-phenomenological perspective. The Lancet Psychiatry, 8(3), 237-249.
- Freeman, D., Garety, P. A., Kuipers, E., Fowler, D., & Bebbington, P. E. (2002). A cognitive model of persecutory delusions. British Journal of Clinical Psychology, 41(4), 331-347.
- González-Rodríguez, A., Guàrdia, A., Palao, D. J., Labad, J., & Seeman, M. V. (2020). Moderators and mediators of antipsychotic response in delusional disorder: Further steps are needed. World journal of psychiatry, 10(4), 34–45. https://doi.org/10.5498/wjp.v10.i4.34
- Goodwin, F. K., & Jamison, K. R. (2007). Manic-depressive illness: bipolar disorders and recurrent depression (Vol. 2). Oxford university press.
- Kiran, C., & Chaudhury, S. (2009). Understanding delusions. Industrial psychiatry journal, 18(1), 3.
- Knowles, R., McCarthy-Jones, S., & Rowse, G. (2011). Grandiose delusions: A review and theoretical integration of cognitive and affective perspectives. Clinical Psychology Review, 31(4), 684-696.
- Joseph SM, Siddiqui W. Delusional Disorder. [Updated 2022 Jul 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
- Langdon, R., & Coltheart, M. (2000). The cognitive neuropsychology of delusions. Mind & Language, 15(1), 184-218.
- Mehl, S., Werner, D., & Lincoln, T. M. (2015). Does Cognitive Behavior Therapy for psychosis (CBTp) show a sustainable effect on delusions? A meta-analysis. Frontiers in psychology, 1450.
- Pawar, A., Mullins, S., & Spence, S. A. (2002, January). Dissecting psychotic phenomenology: Thought broadcasting. In Schizophrenia Research (Vol. 53, No. 3, pp. 64-65).
- Wilson, J. E., Mart, M. F., Cunningham, C., Shehabi, Y., Girard, T. D., MacLullich, A. M., … & Ely, E. W. (2020). Delirium. Nature Reviews Disease Primers, 6(1), 90.
Are You a Therapist, Coach, or Wellness Entrepreneur?
Grab Our Free eBook to Learn How to Grow Your Wellness Business Fast!